


 i_need_contribute
i_need_contribute
Acupuncture reduced migraine frequency and headache-related disability in patients with migraine without aura in a randomized clinical trial. Patients receiving acupuncture experienced greater reductions in monthly migraine days, headache days, pain intensity, and acute medication use compared with a sham acupuncture control. The study also identified baseline brain connectivity patterns associated with clinical response to acupuncture therapy, providing both clinical and neurobiological evidence supporting acupuncture treatment for migraine without aura.
The trial enrolled 120 adults aged 18–65 years diagnosed with migraine without aura according to the International Classification of Headache Disorders, third edition. The study was conducted at Beijing Hospital of Traditional Chinese Medicine, Capital Medical University in China. Participants were randomly assigned to receive either real acupuncture or sham acupuncture following a baseline assessment period. Treatments consisted of twelve acupuncture sessions administered over four weeks, with three sessions weekly, ideally scheduled every other weekday. Patients recorded migraine frequency, duration, pain intensity, and medication use in standardized headache diaries throughout the treatment period. [1]
Clinical outcomes demonstrated measurable improvements following acupuncture treatment. Patients receiving acupuncture experienced greater reductions in monthly migraine days compared with the sham acupuncture group during the four-week treatment period. Improvements were also observed in monthly headache days, pain intensity measured using the visual analog scale (VAS), and days requiring acute migraine medication. Headache-related disability measured by the Headache Impact Test (HIT-6) also improved more in the acupuncture group. Quality-of-life scores measured with the Migraine-Specific Quality of Life Questionnaire improved across three domains including role function-restrictive, role function-preventive, and emotional function.
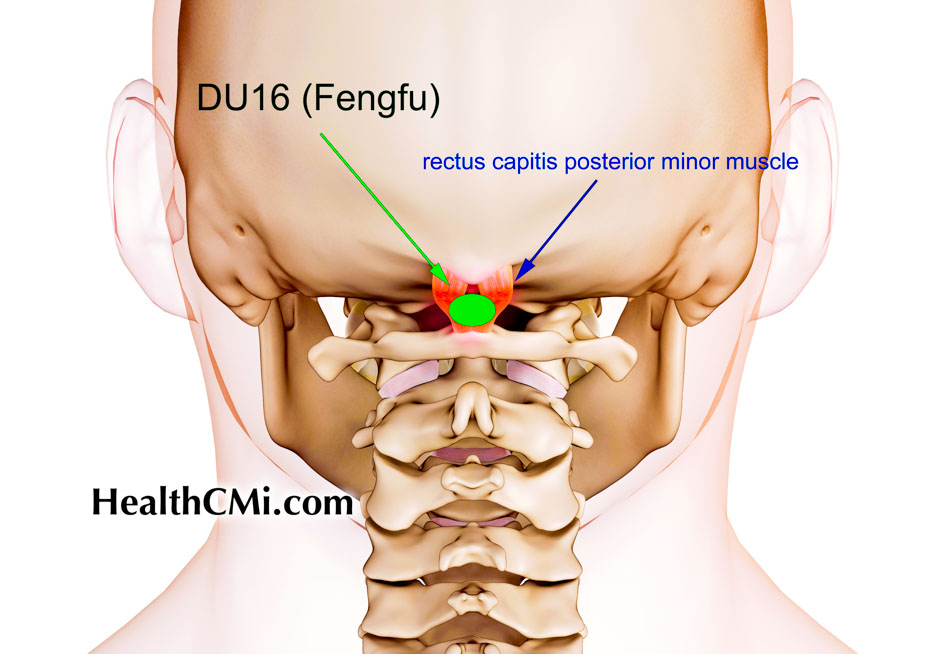
The acupuncture intervention used a standardized point prescription. Eight acupoints were selected: Baihui (GV20), Fengfu (GV16), bilateral Fengchi (GB20), bilateral Taiyang (EX-HN5), and bilateral Hegu (LI4). Treatments were administered by licensed acupuncturists with a minimum of five years of clinical experience. Disposable Hwato acupuncture needles measuring 0.25–0.30 mm in diameter and 25–40 mm in length were inserted at the selected points. After insertion, practitioners applied manual needle stimulation including twirling, lifting, and thrusting techniques to elicit deqi sensation. In the study, deqi was defined as characteristic sensations including distention, numbness, soreness, or radiating sensations perceived during needle manipulation. Each treatment session lasted 30 minutes. [1]
The control group received superficial needling at eight non-acupuncture locations not situated on recognized meridians. Needle manipulation was performed similarly to the real acupuncture protocol but without eliciting deqi sensation. Both treatment groups received identical treatment frequency and treatment duration. This study design allowed investigators to distinguish the physiological effects of acupuncture point stimulation from nonspecific needling effects.
This type of control group remains controversial yet informative in acupuncture research. In this study, the control group received superficial needling at non-meridian locations with needle manipulation performed without eliciting deqi sensation. Such sham acupuncture designs attempt to control for placebo effects and patient expectations while preserving the appearance of treatment. However, superficial needling itself may produce physiological stimulation, meaning the control intervention may not be biologically inert. As a result, comparisons between real and sham acupuncture can provide valuable insight into the specific effects of acupuncture point stimulation and deqi elicitation, while also highlighting the methodological challenges inherent in designing placebo controls for acupuncture clinical trials.
Researchers also evaluated neurological mechanisms associated with acupuncture treatment using resting-state functional magnetic resonance imaging (fMRI). Investigators applied connectome-based predictive modeling, a computational method that analyzes functional connectivity across the brain to identify patterns associated with treatment response.
Analysis revealed that baseline brain connectivity patterns predicted improvements in pain intensity and headache-related disability following acupuncture treatment. Reduced connectivity between the default mode network and subcortical-cerebellar regions was associated with greater reductions in VAS pain scores. Increased connectivity between subcortical-cerebellar structures and motor networks predicted greater improvements in HIT-6 disability scores. Predictive modeling did not identify significant associations for monthly migraine days, monthly headache days, acute medication use days, or quality-of-life scores, indicating that the identified neuroimaging markers were specifically associated with pain intensity and disability rather than migraine frequency.
Further analysis identified specific brain regions associated with treatment response. Nodes associated with reductions in pain intensity were located primarily in the limbic system, prefrontal cortex, putamen, and occipital lobe. Nodes associated with improvements in headache-related disability were concentrated in the caudate nucleus, hippocampus, thalamus, motor cortex, prefrontal cortex, and cerebellum. These brain regions are involved in pain perception, emotional regulation, and sensorimotor processing. The authors noted that baseline connectivity patterns likely reflect a predisposition to respond to acupuncture rather than a direct causal mechanism. [1]
Adverse events associated with acupuncture were mild and uncommon. Five patients (4.2 percent) in the acupuncture group reported minor adverse events including subcutaneous hematoma, needling pain, and localized numbness. The same number of adverse events occurred in the sham acupuncture group, and no significant difference between groups was observed. No serious adverse events were reported.
The investigators concluded that acupuncture produced measurable improvements in migraine symptoms and headache-related disability. Neuroimaging findings further suggested that baseline brain connectivity signatures may help identify patients most likely to benefit from acupuncture therapy, supporting the potential for individualized treatment strategies based on neurological biomarkers. [1]
Source
1. Xinyu Zhang et al. Acupuncture for Migraine Without Aura and Connection-Based Efficacy Prediction: A Randomized Clinical Trial. JAMA Network Open. 2026.





 Research
Research
